
You might not expect your period to cause back pain, but many people feel it every cycle. Menstrual back pain usually comes from uterine cramps and hormone-driven inflammation that refers pain to your lower back, and simple steps can ease it. This article explains the biology behind that pain and shows practical ways to find relief.
You will learn how doctors tell menstrual back pain apart from other conditions, which treatments have solid evidence, and which alternative approaches may help. Use these clear strategies to reduce pain now and lower the chance it returns in future cycles.
Understanding Menstrual Pain
You may feel cramping, pressure, and aches in your lower belly and back during your period. Knowing the different types of pain, common symptoms, and medical terms helps you recognize what’s normal and when to seek help.
Types of Menstrual Discomfort
Primary dysmenorrhea is the common crampy pain caused by uterine contractions. It usually starts a few hours before or when bleeding begins and peaks in the first 24–48 hours. Pain often spreads to the lower back and thighs and can range from mild to severe.
Secondary dysmenorrhea comes from an underlying condition, like endometriosis, fibroids, or pelvic inflammatory disease. Pain may begin earlier in the cycle, last longer, or feel different from your usual cramps. You might also notice pain outside your period or changes in bleeding.
Other types include ovulatory pain (mittelschmerz) and non-menstrual pelvic pain that coincides with your cycle. Identify patterns: timing, location, triggers, and response to over-the-counter medicine. That helps your clinician recommend targeted tests or treatments.
Common Symptoms Associated With Periods
Cramping is the most common symptom, felt as dull or sharp spasms in the lower abdomen. You may also have steady aching in the lower back that worsens with movement or prolonged standing.
You might experience heavy or irregular bleeding, which can increase fatigue and make pain feel worse. Nausea, headache, diarrhea, and lightheadedness often occur with strong cramps because prostaglandins affect other organs.
Note when symptoms start and how long they last. Track pain severity, medicines that help, and any extra signs like fever or extreme fatigue. This record helps your healthcare provider decide if tests or treatments are needed.
Medical Terminology for Menstrual Pain
Dysmenorrhea means painful menstruation. Primary dysmenorrhea has no identifiable pelvic disease and is linked to prostaglandin-driven uterine contractions.
Secondary dysmenorrhea refers to pain from a condition such as endometriosis (uterine-like tissue outside the uterus), uterine fibroids (benign muscle growths), or adenomyosis (uterine lining grows into the muscle). Each condition changes pain timing, location, and response to treatment.
Prostaglandins are hormones that trigger uterine muscle tightening and inflammation, causing cramping and sometimes nausea or diarrhea. Knowing these terms lets you describe symptoms clearly to a clinician and understand suggested treatments.
Biological Causes of Back Pain During Menstruation
You may feel back pain during your period for specific biological reasons. Hormone shifts, body inflammation, and chemical signals from the uterus each play a clear role.
Hormonal Fluctuations and Muscle Tension
Your estrogen and progesterone levels fall just before and during your period. That drop can increase muscle tension in your lower back and pelvic area. Muscles tighten because hormone changes affect nerve signals and your pain threshold.
Reduced estrogen can also affect fluid balance and connective tissue elasticity. That makes muscles and ligaments stiffer, so normal movement feels more uncomfortable. You might notice soreness when you stand, sit, or bend.
Hormone-linked mood changes can increase how much pain you feel. Stress raises muscle tension and makes pain feel worse than it would when you are relaxed.
Inflammatory Responses in the Body
Your immune system releases inflammatory molecules around the time of your period. These include cytokines and other immune signals that increase local swelling and sensitivity. Inflammation can spread from the uterus to nearby pelvic tissues and the lower back.
Inflammatory chemicals sensitize nerves, so normal sensations register as pain. You may feel a deep, aching pain that matches the timing of bleeding and cramps. Anti-inflammatory medicines help because they lower these signals and reduce nerve sensitivity.
Lifestyle factors, such as poor sleep or high stress, can make inflammation stronger. Managing these factors often reduces the intensity of your back pain.
Prostaglandin Effects on the Uterus and Back
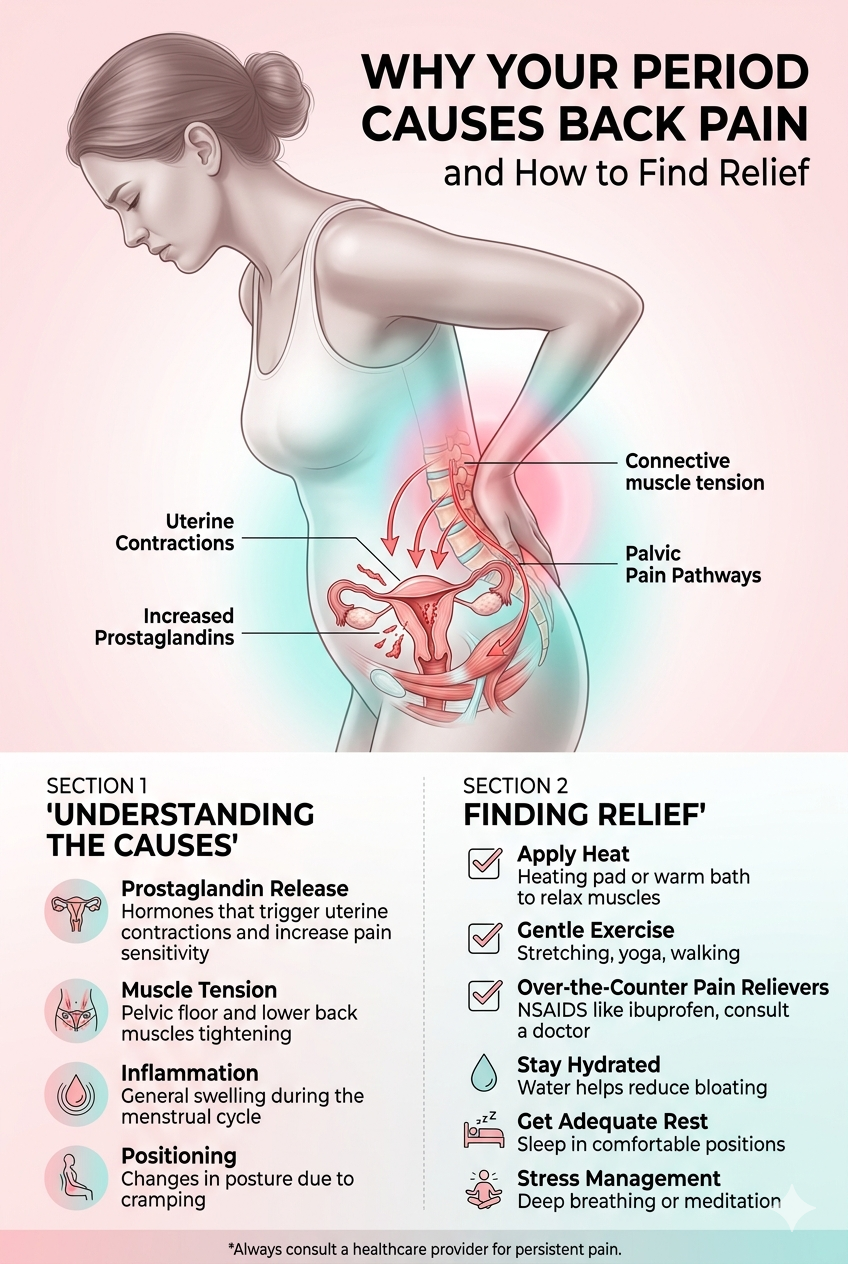
Your uterus produces prostaglandins to trigger contractions that expel its lining. High prostaglandin levels cause stronger uterine contractions and more pain. Those contractions can refer pain to your lower back through shared nerve pathways.
Prostaglandins also cause nearby blood vessels to constrict and then dilate, which increases pain and discomfort. When levels are high, you may get cramping that starts in your pelvis and radiates to your lumbar region.
Nonsteroidal anti-inflammatory drugs (NSAIDs) lower prostaglandin production and often ease both cramps and back pain. If NSAIDs do not help, talk to your clinician about other options.
When Back Pain Signals an Underlying Condition
Some back pain during your period is normal, but certain signs mean a deeper issue. Watch for worsening pain, pain that starts before your period, pain that won’t respond to usual treatments, or pain with other symptoms like heavy bleeding or bowel changes.
Endometriosis and Its Impact
Endometriosis happens when tissue similar to your uterine lining grows outside the uterus. This tissue responds to your hormones and bleeds each cycle, causing inflammation, scar tissue, and painful adhesions. If implants are on ligaments, ovaries, or the pelvic lining, you may feel sharp or deep pain in your lower back that can start before your period and last days after it ends.
You might also have very heavy periods, pain during sex, or trouble getting pregnant. Doctors use pelvic exams, ultrasound, or laparoscopy to diagnose it. Treatments include hormonal birth control, GnRH agonists, or surgery to remove lesions. Pain meds and pelvic physical therapy can help manage symptoms while you seek a diagnosis.
Reproductive System Disorders
Other reproductive issues can cause back pain. Uterine fibroids, especially when large or located on the back wall of the uterus, press on nearby nerves and produce dull, heavy back pain. Adenomyosis, where uterine tissue grows into the muscle wall, leads to cramping and lower back ache that worsens with your period.
Pelvic inflammatory disease (PID) from infection can cause constant, severe lower back and pelvic pain, often with fever, abnormal discharge, or painful urination. Ovarian cysts can cause sudden, one-sided back or pelvic pain if they twist or rupture. Your doctor may recommend ultrasound, pelvic exam, antibiotics for infections, hormonal treatments, or surgery depending on the cause.
Musculoskeletal Factors Affecting Pain
Muscle tightness and joint problems can make menstrual back pain worse. Your pelvic floor muscles may tighten from menstrual cramps, causing referred pain to the lower back. Poor posture, weak core muscles, and lumbar spine arthritis or disc issues can amplify period-related pain.
Physical therapists use stretching, soft-tissue release, and strengthening to ease pelvic floor and lower back tension. Heat, targeted exercise, and posture correction often reduce pain. If a spinal condition contributes, imaging and specialist care may be needed to treat the root problem and prevent recurring menstrual back pain.
Diagnosing Menstrual Back Pain
You may need to track your pain, describe it clearly, and get basic tests to find causes like cramps, endometriosis, or a spine issue. The steps below explain what clinicians look for and when you should get help.
Professional Evaluation of Symptoms
A clinician will ask you about pain timing, location, and pattern. Expect questions such as: when the pain starts in relation to your period, whether it is dull or sharp, how long it lasts, and what makes it better or worse.
You should bring a symptom diary showing at least three cycles. Note pain intensity (0–10), bleeding amount, medicine you used, activity limits, and any bowel or urinary changes. Also list past pelvic surgeries and family history of conditions like endometriosis.
The provider will do a focused exam of your abdomen, pelvis, and lower back. They will check for pelvic tenderness, uterine size, pelvic masses, and spinal range of motion. Findings guide the next steps and help rule in or out gynecologic versus musculoskeletal causes.
Diagnostic Tests and Procedures
Imaging often starts with pelvic ultrasound to look for fibroids, cysts, or signs of endometriosis-related masses. Ultrasound is noninvasive and commonly available. It may be transabdominal or transvaginal depending on what needs evaluation.
If ultrasound is normal but symptoms persist, your clinician might order MRI of the pelvis or lower spine. MRI gives better detail for soft tissues and can detect deep endometriosis or spinal disc problems. CT scans are less common for menstrual causes.
Lab tests may include pregnancy test, complete blood count for anemia, and inflammatory markers if infection is suspected. If endometriosis is likely and symptoms are severe, diagnostic laparoscopy may be recommended to directly view and treat lesions.
When to Seek Medical Advice
See a clinician if pain stops you from doing usual activities or requires opioid or frequent NSAID use. Also get help for fever, heavy bleeding soaking a pad/hour, fainting, or signs of infection like severe pelvic tenderness with fever.
Seek prompt care if back pain is asymmetric with leg numbness or weakness, or if you have new bladder or bowel dysfunction. These signs may point to a spinal emergency or nerve compression requiring urgent evaluation.
If you notice a clear pattern across cycles that worsens over time, request referral to a gynecologist. Early evaluation helps identify treatable conditions like endometriosis, fibroids, or structural spine issues.
Evidence-Based Relief Strategies
You can ease period-related back pain with medicines, targeted movement, daily habit changes, and simple tools. Each method helps in a different way, so pick what fits your pain level and lifestyle.
Pharmacological Treatments
Use NSAIDs like ibuprofen (200–400 mg every 4–6 hours) or naproxen (220 mg every 8–12 hours) as first-line treatment. Start at the first sign of cramps or back pain and follow package directions. These reduce prostaglandins that cause uterine cramps and referred back pain.
If NSAIDs do not help, your doctor may prescribe acetaminophen or a stronger pain reliever for short-term use. For heavy bleeding with pain, hormonal options like combined oral contraceptives or levonorgestrel IUDs can reduce cycle pain over months. Watch for side effects: stomach upset, bleeding changes, or medication interactions, and avoid NSAIDs if you have ulcers, bleeding disorders, or certain heart/kidney problems.
Ask your clinician about muscle relaxants or short courses of prescription pain meds only if other measures fail. Always follow dosing limits and discuss safe use if you smoke, are pregnant, or take other drugs.
Physical Therapy Techniques
Do pelvic and lumbar stretching to reduce tightness that drives back pain. Try a daily routine: knee-to-chest stretch (30 seconds each side), child’s pose (30–60 seconds), and supine pelvic tilts (10–15 reps). Move slowly and breathe deeply during each stretch.
Strengthen core and glute muscles to support your lower back. Simple exercises include bridges (3 sets of 10), bird-dog (8–12 reps per side), and planks (20–60 seconds). Start with low intensity and increase as pain allows.
Use heat on sore areas for 15–20 minutes to relax muscles before exercise. A physical therapist can give hands-on techniques, tailored exercise plans, and advice on posture and movement patterns that reduce pain during your period.
Lifestyle Adjustments for Pain Management
Sleep, hydration, and diet affect inflammatory pain. Aim for 7–9 hours of sleep and drink plenty of water to reduce cramping intensity. Cut back on high-sodium foods and limit caffeine and alcohol during your period if they worsen cramps.
Apply a regular low-impact exercise schedule. Walk briskly 20–30 minutes most days or do gentle yoga to increase blood flow and reduce pain. Exercise releases natural pain-relieving chemicals called endorphins.
Manage stress with breathing exercises or short meditations. Try diaphragmatic breathing for 5 minutes each morning and evening. Track your cycle and symptoms in a simple app or diary to spot patterns and plan treatment beforehand.
Supportive Devices and Tools
Use a heating pad or heat patch on the lower back or pelvis to reduce muscle spasm and pain. Choose dry heat for 15–20 minutes; use patches for up to 8–12 hours if needed. Avoid high settings to prevent burns.
Consider over-the-counter TENS units for short-term relief. Place electrodes on the lower back following device instructions and use for 20–30 minutes. TENS can reduce pain signals without medication for some people.
Supportive cushions and ergonomic chairs help when you sit for long periods. Use a lumbar roll or small pillow to maintain natural spine curve. A firm mattress and pillow that keep your spine aligned can lessen morning soreness.