
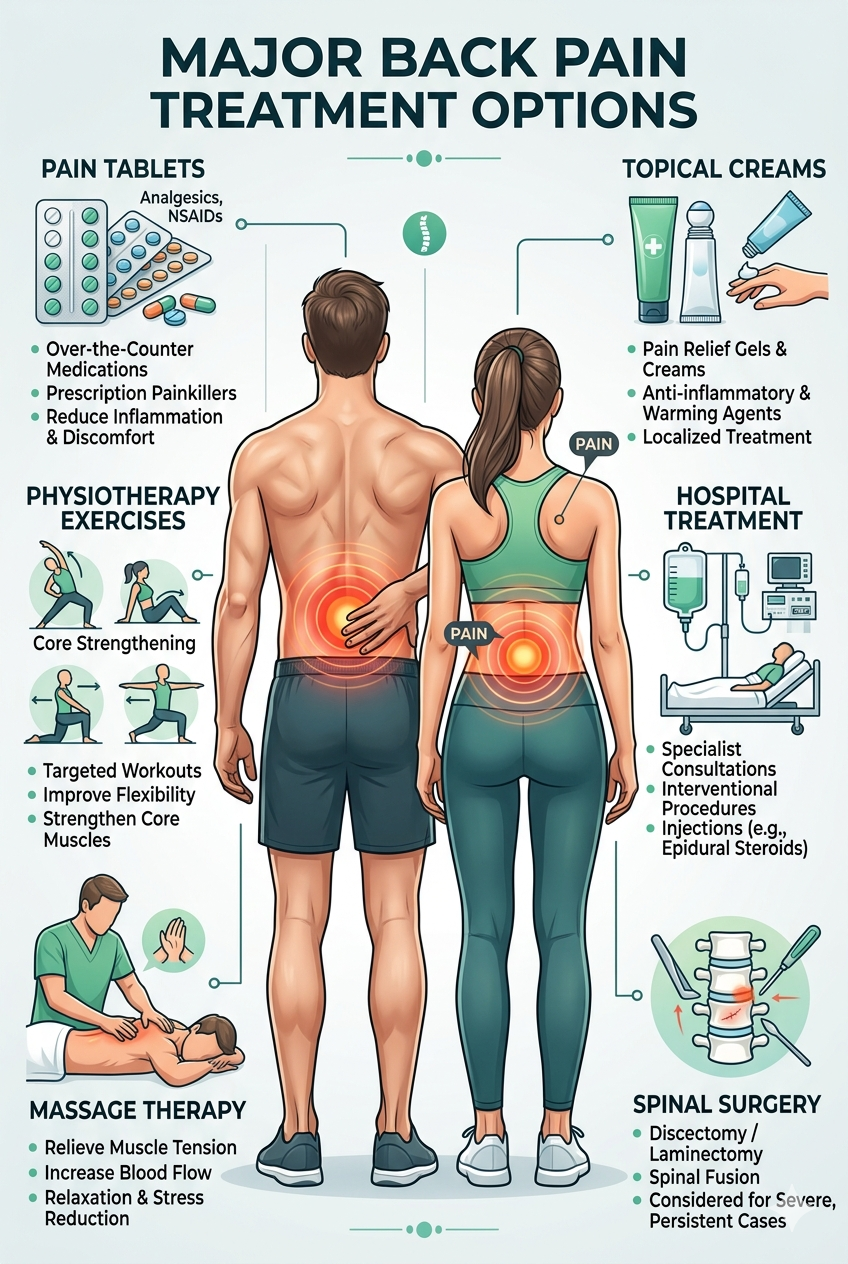
Back pain can come from many causes, and you have several treatment paths to choose from. You can often ease pain with pills, creams, physiotherapy, or massage, while more severe cases may need hospital care or surgery.
This article guides you through non-surgical options like exercise and hands-on therapy, when to try topical or oral medications, and when to seek advanced medical care. You will learn how to match treatments to your situation and how to prevent future episodes.
What Causes Back Pain?
Back pain can come from injured muscles, worn spinal parts, nerve pressure, or medical conditions. Your age, job, and activity level shape how and why pain starts and how it affects daily tasks.
Primary Causes and Risk Factors
You can get back pain from muscle strains when you lift objects incorrectly or twist suddenly. Repeated bending, heavy lifting, and poor posture at work or school increase your risk.
Degenerative disc disease and osteoarthritis wear down spinal discs and joints over years. These changes narrow spaces around nerves and cause pain, numbness, or weakness.
Herniated discs press on nearby nerves after sudden injury or gradual strain. Sciatica describes pain radiating down one leg when the sciatic nerve is pinched.
Other medical causes include spinal stenosis, infections, fractures from osteoporosis, and inflammatory conditions like ankylosing spondylitis. Smoking, obesity, and low fitness make healing slower and raise your chance of chronic pain.
Symptoms and Diagnosis
Pain location often guides diagnosis: lower back pain points to lumbar issues, neck pain suggests cervical problems. You may feel sharp stabbing pain, dull aching, burning, or tingling. Pain that radiates into your buttocks or legs often signals nerve involvement.
Doctors ask about pain onset, activity that provoked it, and what makes it better or worse. They check posture, spine movement, muscle strength, reflexes, and sensation.
Imaging tests include X-rays for bone problems, MRI for soft tissue like discs and nerves, and CT scans for detailed bone views. Blood tests and nerve studies (EMG) help rule out infection, inflammatory disease, or nerve damage. Red flags—fever, unexplained weight loss, severe weakness, or bowel/bladder changes—need urgent evaluation.
Impact on Daily Living
Back pain can limit your ability to sit, stand, or walk for long periods. You may have trouble dressing, lifting grocery bags, or playing with children. Sleep often suffers when pain worsens at night, which affects mood and concentration.
Work performance drops if your job requires physical tasks or long sitting. You might avoid social activities and exercise, which slows recovery. Pain that lasts more than three months can lead to anxiety and depression, so addressing both physical and emotional aspects helps you return to normal routines.
Non-Surgical Approaches
You can try medicines, hands-on treatments, creams, and changes to daily habits to reduce pain and improve function. These options work together: drugs ease pain, therapy restores movement, and lifestyle shifts prevent flare-ups.
Pharmacological Interventions
You will often start with over-the-counter pain relievers. Acetaminophen reduces mild pain but does not lower inflammation. NSAIDs (ibuprofen, naproxen) reduce pain and swelling; use the lowest effective dose for the shortest time and watch for stomach, kidney, or blood pressure issues.
Your doctor may prescribe stronger medicines for short periods. Muscle relaxants can help spasms but cause drowsiness. Short courses of opioids are rarely used and carry addiction and side-effect risks; use them only if other options fail and with close monitoring.
For nerve-related pain, your clinician may give antidepressants (duloxetine) or antiepileptics (gabapentin) to reduce burning or tingling. Always tell your provider about other medicines and health problems; interactions and side effects matter.
Physical Therapy Benefits
You can learn specific exercises to strengthen core and back muscles that support your spine. A therapist teaches posture correction, flexibility moves, and progressive strengthening so you regain control and reduce strain.
Therapists use hands-on techniques such as manual mobilization, soft-tissue work, and traction to improve joint and muscle function. They may add education on body mechanics to help you lift, sit, and stand safely at work and home.
Physical therapy also uses measured progress. You follow a plan with clear goals—reduce pain, return to activities, or avoid surgery. Regular sessions plus home exercises give the best results.
Topical and Oral Treatments
Topical creams and patches let you apply medicine directly to the painful area. NSAID gels, lidocaine patches, and capsaicin creams offer targeted relief with fewer systemic effects. Apply as directed and check skin for irritation.
Oral options include the drugs mentioned earlier and supplements some people try. Vitamin D and calcium support bone health if you are deficient. Evidence for glucosamine or herbal supplements is mixed; talk to your clinician before starting them.
Combine topical and oral treatments only under guidance to avoid overdosing on the same drug class. Read labels and follow dosing limits, especially for acetaminophen and NSAIDs.
Lifestyle Modifications
You can reduce back pain flare-ups by changing daily habits. Lose excess weight to lower spine load, and stop smoking to improve blood flow and healing. Small changes add up.
Adjust your work and home setup. Use an ergonomic chair, keep your computer screen at eye level, and lift with your legs, not your back. Break long sitting or standing tasks into short movement breaks.
Add regular low-impact exercise such as walking, swimming, or cycling to improve endurance and flexibility. Prioritize sleep and stress management; poor sleep and high stress make pain worse.
Manual and Physical Modalities
You will learn hands-on methods and simple tools that reduce pain, improve motion, and support daily activity. These approaches include specific massage moves, timed heat and cold use, and devices that change how you sit, stand, or move.
Massage Techniques
Massage can ease muscle tightness and reduce nerve irritation when done correctly. Ask a licensed massage therapist or physiotherapist for techniques such as myofascial release, trigger-point work, and deep tissue massage focused on the lower back and gluteal muscles. Expect sessions of 10–30 minutes on specific tight spots, not full-body relaxation.
You should tell the therapist about sharp pain, recent injury, or numbness. They will use moderate pressure and adjust based on your pain level. Home self-massage tools—foam rollers, lacrosse balls, or handheld massagers—help maintain gains between visits. Use slow rolls for 30–60 seconds per spot and stop if pain worsens.
Some people feel short-term soreness after treatment; this usually fades within 24–48 hours. Massage does not fix structural problems like large herniated discs, but it often complements exercise and posture work to reduce symptoms.
3 Back Pain Massage Hacks That Help You Feel Better Naturally
These techniques help reduce cortisol levels, block pain signals, and increase circulation to speed up recovery.
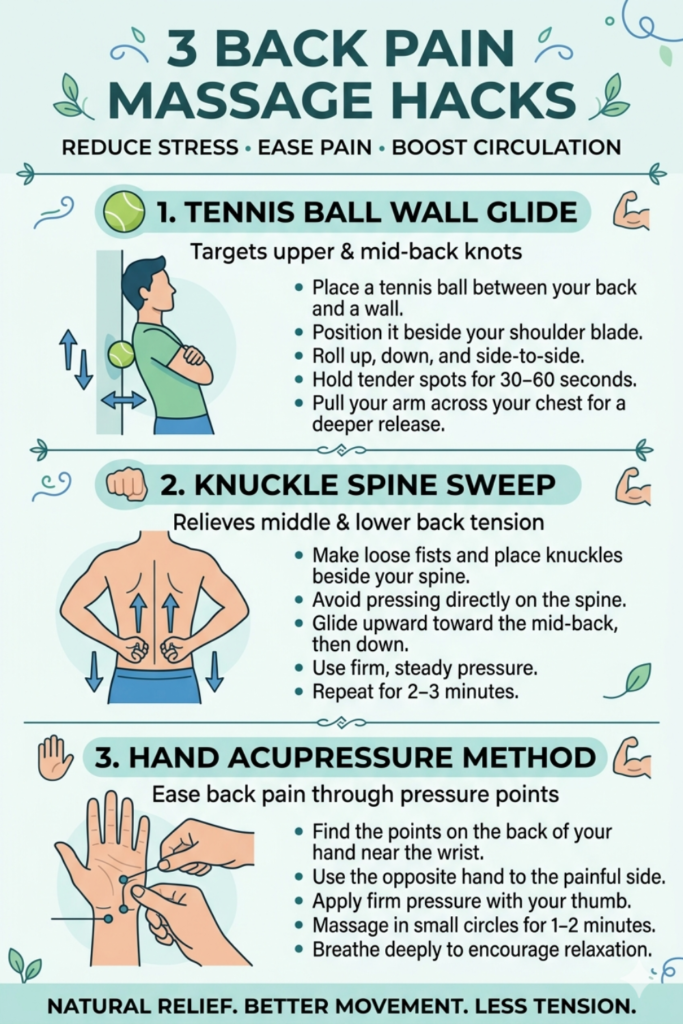
1. The Tennis Ball Wall Glide (Upper & Mid-Back)
This technique allows you to target stubborn muscle knots between your spine and your shoulder blade without straining your arms.
- The Setup: Place a tennis ball, lacrosse ball, or soft massage ball against a wall just below shoulder level.
- The Action: Lean your upper back against the ball, positioning it right inside your shoulder blade.
- The Pressure: Move your feet further from the wall to increase the intensity.
- The Movement: Gently roll your body up, down, and side-to-side to find a sensitive “trigger point”.
- The Release: Hold your position on that spot for about one minute while pulling your arm across your chest to let the deep muscles completely let go.
2. The Knuckle Spine Sweep (Middle & Lower Back)
You can easily massage your own lower and middle back using your knuckles to stimulate deep tissue layers.
- The Setup: Stand up straight with your feet hip-width apart.
- The Hand Position: Form loose fists with both hands and reach around to the back of your waist.
- The Alignment: Place your knuckles firmly on the thick muscle bands on either side of your spine. Never press directly onto the spinal bones.
- The Stroke: Apply firm, steady pressure and slowly glide your knuckles upward toward your mid-back, then back down to your hips.
- The Loop: Repeat this upward sweeping motion for two to three minutes to promote local blood flow.
3. The Hand Acupressure Method (Remote Back Relief)
According to Traditional Chinese Medicine (TCM), you can relieve severe lower back strain without touching your back at all by targeting a remote pressure point on your hand.
- The Point: Locate the Yao Tong Xue acupressure points on the back of your hand, found in the depressions between the bones just below your wrist.
- The Strategy: Always treat the hand opposite to the side of your back pain (e.g., massaged the left hand if the right side of your lower back hurts).
- The Action: Use your thumb or the eraser end of a pencil to apply deep, firm pressure into the groove.
- The Micro-Movement: Gently rub the point in small circles for one to two minutes while taking deep breaths to signal your nervous system to relax.
Heat and Cold Therapy
Use cold (ice) for the first 24–72 hours after a new injury to reduce swelling and sharp pain. Apply a cold pack wrapped in cloth for 10–20 minutes every 1–2 hours. Avoid direct skin contact to prevent frostbite.
Switch to heat when pain becomes more chronic or stiffness persists. Use a warm pad or hot pack for 15–20 minutes to relax muscles before stretching or exercise. You can also use moist heat from a warm shower or towel.
Combine heat before activity and cold after activity for best effect. Do not use heat on swollen or inflamed areas. Check skin regularly and stop therapy if you have poor sensation, diabetes, or circulatory problems without medical approval.
Assistive Devices
Assistive devices change how your spine carries weight and can reduce pain during daily tasks. Common options include lumbar support belts, seat cushions with lumbar contour, adjustable standing desks, and walking sticks for short-term relief after flare-ups. Choose devices that fit your body and let you maintain a neutral spine.
Use lumbar pillows to keep the lower back supported while sitting; look for a 3–5 cm curve that matches your natural lordosis. For lifting tasks, use a rigid back brace only temporarily and combine with proper lifting technique—bend knees, keep load close to your body.
Work with a physiotherapist or occupational therapist to select and fit devices. Improper use can worsen pain or cause dependency, so learn correct use and aim to wean off supports as your strength and movement improve.
Advanced Medical Interventions
These treatments act when simpler care has not helped. They include image-guided injections, targeted surgeries, and supervised inpatient rehab to relieve pain and restore function.
Minimally Invasive Procedures
Minimally invasive procedures use small needles or tiny incisions to treat specific causes of back pain. You may get an epidural steroid injection for nerve inflammation, a facet joint injection for joint pain, or a nerve block to diagnose and treat pain sources. These are often done with fluoroscopy or CT guidance so the doctor places medicine precisely.
Radiofrequency ablation uses heat to interrupt pain signals from small nerves. It can give months of relief for facet-mediated pain. Percutaneous discectomy or endoscopic discectomy removes part of a herniated disc through a small tunnel when a clear disc fragment presses a nerve. Risks include infection, bleeding, and temporary nerve irritation. Recovery is usually quicker than open surgery, but success depends on correct diagnosis and patient selection.
Surgical Options
Surgery aims to fix structural problems that cause persistent pain or neurological deficits. Common procedures include lumbar decompression (laminectomy or microdecompression) to release nerve pressure and fusion to stabilize unstable vertebrae. Artificial disc replacement is an option for some disc cases to preserve motion.
You should expect preoperative imaging, discussions about risks (infection, nerve injury, blood loss), and a plan for post-op rehab. Recovery time varies: decompression can allow return to light activity in weeks; fusion may take months for bone healing. Surgeons assess your overall health, pain pattern, and imaging to recommend the best procedure. Outcomes improve when you follow rehab and activity guidelines after surgery.
Hospital-Based Rehabilitation
Hospital-based rehab offers a structured program when pain limits daily life or after surgery. You receive coordinated care from physicians, physical therapists, occupational therapists, and pain nurses. Programs include graded exercise, gait training, posture education, and pain management strategies tailored to your needs.
Therapists progress intensity based on pain and function. You may also get cognitive-behavioral support to cope with chronic pain and learn activity pacing. Inpatient or outpatient stays focus on measurable goals: improve walking distance, reduce opioid use, or return to work. Regular reassessments guide the plan and adjust treatments like aquatic therapy, electrical stimulation, or specialized bracing.
Choosing Suitable Therapies
You should match treatments to your pain cause, severity, and daily needs. Think about how each option affects work, mobility, recovery time, and costs.
Personalized Treatment Planning
You need a plan based on your exact diagnosis, symptoms, and goals. Start with clear tests: physical exam, pain mapping, and imaging only if needed. Use this info to choose from tablets, physiotherapy, massage, topical creams, injections, or surgery.
List your priorities: pain relief, return to work, avoiding surgery, or fast recovery. Ask about expected timelines and side effects for each choice. Make stepwise plans — try conservative care first (medication, exercise, manual therapy) and move to injections or surgery if pain persists. Review progress every 4–8 weeks and adjust medicines, therapy intensity, or consider specialist referral if you do not improve.
Multidisciplinary Care Teams
You benefit from a team when your pain is complex or long-lasting. A typical team includes your primary doctor, a physiotherapist, a pain specialist, and sometimes a surgeon or psychologist. Each professional brings a specific role: medicines and diagnosis from the doctor, exercise and movement retraining from the physiotherapist, procedures from the pain specialist, and surgery assessment from the surgeon.
Coordinate care with one lead clinician to avoid conflicting advice. Use shared notes or a care plan listing current treatments, who manages each part, and next review dates. Expect regular team reviews when recovery stalls or when you consider invasive options.
Prevention and Long-Term Management
Build habits that protect your back, keep your muscles strong, and catch problems early. Focus on movement, daily care, and regular check-ins to reduce flare-ups and limit pain over time.
Exercise and Mobility Routines
Do strength and flexibility work at least 3 times a week. Include core exercises like planks and bridges, hip glutes moves such as clamshells and hip thrusts, and back extensions. Start with low resistance and increase slowly as you get stronger.
Add daily mobility: gentle cat-cow, pelvic tilts, knee-to-chest, and hamstring stretches for 5–10 minutes. Walk 20–30 minutes most days to keep blood flow and reduce stiffness. If you sit at work, stand and walk for 2–3 minutes every 30–60 minutes.
Use correct form. Keep a neutral spine during lifts, bend at hips and knees, and hold objects close to your body. If you use weights or machines, ask a physiotherapist for tailored progressions and limits.
Self-Care Strategies
Manage pain with targeted actions you can do at home. Use heat for tight muscles (15–20 minutes) and ice for new inflammation (10–15 minutes). Alternate based on what helps you feel better.
Maintain a healthy weight to reduce load on the spine. Follow a balanced diet with protein, calcium, and vitamin D. Avoid smoking; it impairs disc health and slows healing.
Adjust your environment: set your chair so hips are slightly higher than knees, keep monitors at eye level, and use a lumbar roll if needed. For sleep, choose a mattress and pillow that keep your spine neutral.
Use over-the-counter pain relievers as directed for short-term relief. Apply topical analgesic creams for localized pain. See a clinician before long-term medication use.
Monitoring and Follow-Up
Keep a pain and activity log for 2–4 weeks to spot triggers. Note activity, pain level (0–10), duration, and what eased symptoms. Share this with your clinician to guide treatment changes.
Schedule follow-ups with your physiotherapist or doctor every 6–12 weeks while you build your routine, then at least yearly or when symptoms change. Seek earlier review for increasing pain, numbness, weakness, or loss of bladder/bowel control.
Get imaging only when red flags appear or symptoms persist despite 6–12 weeks of conservative care. Use referral to a spine specialist if conservative care fails, symptoms worsen, or surgery becomes a possible option.
Innovations in Back Care
New devices, smarter drugs, and better rehab tools are changing how back pain is treated. You will find tech that reduces surgery, meds that target nerves, and therapy tools that speed recovery.
Emerging Technologies
You can now access wearable sensors that track your spine position, movement, and muscle activity. These devices give real-time feedback during work or exercise so you can correct posture before pain starts.
Minimally invasive spine surgery uses smaller incisions and tubular retractors. That lowers infection risk, shortens hospital stays, and speeds your return to daily life compared with open surgery.
Neuromodulation—such as spinal cord stimulators and dorsal root ganglion stimulators—can reduce chronic pain by altering nerve signals. Recent models use rechargeable batteries and programmable settings tailored to your pain pattern.
Image-guided injections and robot-assisted needle placement improve accuracy for steroid or biologic injections. Better targeting means fewer repeat procedures and less steroid exposure for you.
Future Trends in Treatment
Biologic therapies aim to repair damaged discs and tissues. Early trials use growth factors, stem cells, or platelet-rich plasma to reduce degeneration. These approaches focus on healing instead of masking pain.
Artificial intelligence will help personalize care. AI can analyze your imaging, activity data, and symptom history to recommend medication doses, physical therapy plans, or the need for referral to a surgeon.
Tele-rehabilitation platforms let you do guided physiotherapy at home with video coaching and progress tracking. This reduces travel and keeps you consistent with exercises that prevent flare-ups.
Smart pills and drug-delivery patches are in development to release pain medicine at controlled rates. These methods could lower side effects and keep levels steady without frequent dosing.