
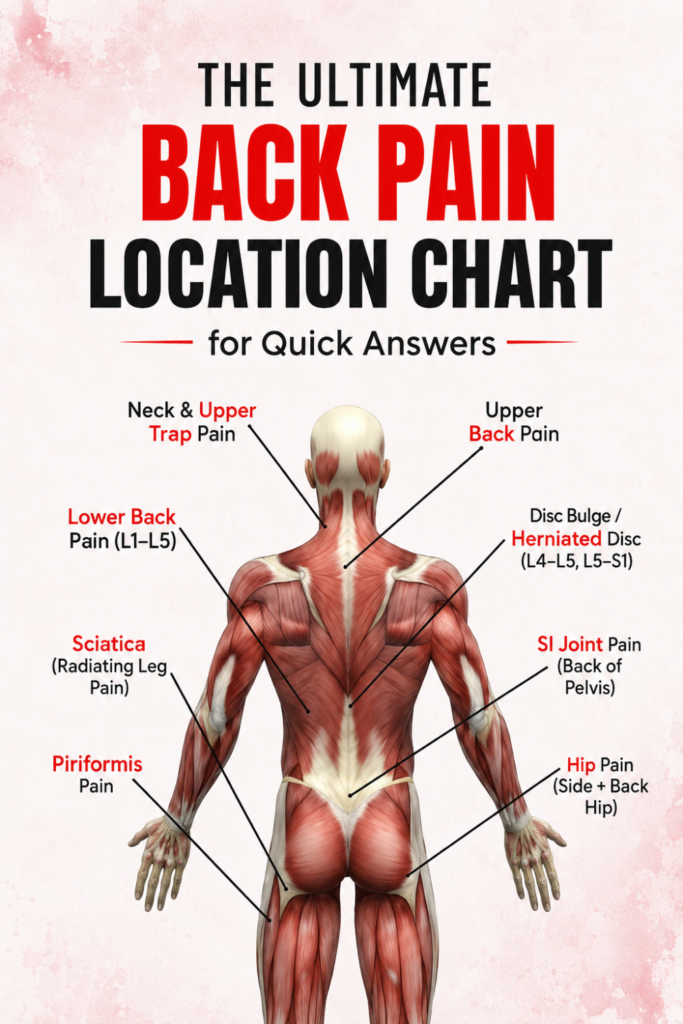
Back pain can come from many places in your spine, muscles, nerves, or internal organs, and the spot that hurts often points to the likely cause. Sharp pain between your shoulder blades usually stems from muscle strain, while numbness or shooting pain down your leg often means a nerve is pinched in your lower spine.
You will learn how spinal bones, discs, joints, nerves, and organs each cause pain in different locations. The guide will also show which symptoms suggest urgent problems and which you can often manage with posture, movement, or simple care.
Understanding Back Anatomy
You will learn where pain can start, which moving parts are involved, and how nerves carry pain signals. These points help you link symptoms to likely causes and guide what to check first.
Regions of the Spine
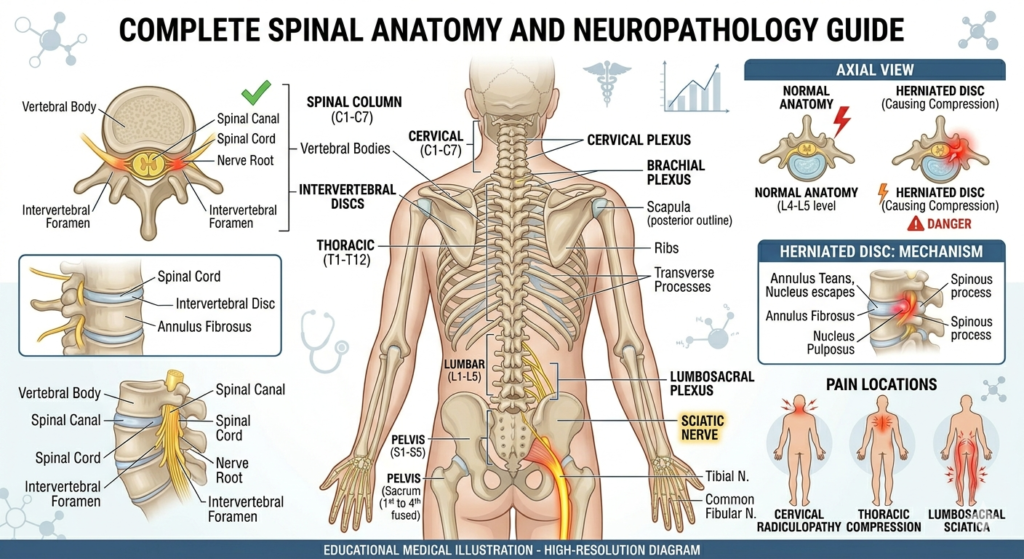
The spine has five main parts: cervical (neck), thoracic (mid-back), lumbar (lower back), sacrum, and coccyx (tailbone). Each part has vertebrae stacked with discs between them that act as shock absorbers.
Cervical vertebrae (C1–C7) support your head and allow rotation and nodding. Thoracic vertebrae (T1–T12) attach to ribs and limit bending. Lumbar vertebrae (L1–L5) bear most body weight and allow bending and lifting.
The sacrum is a triangular bone fused from five segments and connects the spine to the pelvis. The coccyx is small and often painful after falls. Location matters: pain in the neck points to cervical issues, mid-back pain to thoracic problems, and lower back pain most often to lumbar structures.
Major Muscles and Ligaments
Large muscles support posture and movement. The erector spinae group runs along both sides of the spine and helps you stand and extend your back. The multifidus sits deeper and stabilizes each vertebra during small movements.
The quadratus lumborum and psoas connect the spine to the pelvis and legs and affect hip and lower back function. Muscles can strain from overuse, sudden lifts, or poor posture, causing localized pain and tightness.
Ligaments like the anterior longitudinal and posterior longitudinal run along the front and back of vertebrae. They limit excessive motion and keep the spine aligned. Sprains or degeneration of these ligaments reduce stability and can cause pain or contribute to disc problems.
Nerve Pathways
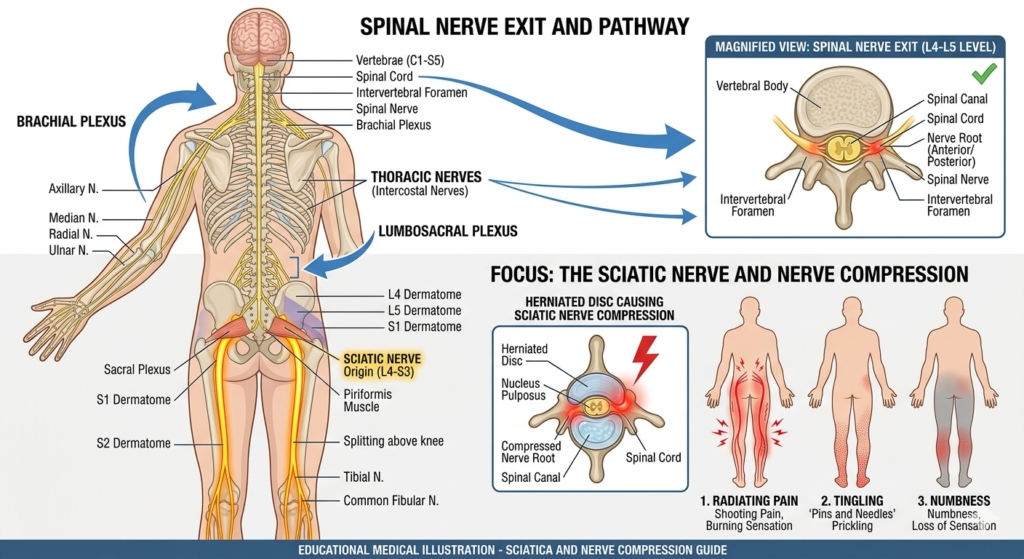
Nerves leave the spinal cord through openings called foramina between vertebrae. Each spinal nerve serves a specific skin area (dermatome) and set of muscles (myotome). Compression or inflammation of a nerve causes pain, numbness, or weakness along that nerve’s path.
The sciatic nerve is the largest and runs from the lower spine down the leg; irritation here causes sciatica—sharp pain, tingling, or weakness in the buttock and leg. Cervical nerve compression can cause pain, numbness, or weakness in the shoulder, arm, or hand.
Common causes of nerve compression include herniated discs, bone spurs from arthritis, and thickened ligaments. You can often trace symptoms by matching where you feel pain to the nerve pathways involved.
Upper Back Pain: Primary Causes
Upper back pain often comes from muscles, posture, or small joints near your spine. Each cause has distinct signs like sharp pain with movement, aching after sitting, or limited twist and reach.
Muscle Strain and Sprain
Muscle strain occurs when fibers in your upper back are overstretched or torn. Common triggers include lifting heavy objects incorrectly, sudden twisting, or sports that stress the shoulders and ribs. You may feel localized pain, tightness, and muscle spasms. Pain usually worsens with certain movements, like reaching overhead or turning your trunk.
Sprains affect the ligaments that connect bones in the upper back and often follow a sudden force or fall. You might notice swelling and tenderness over the affected area. Rest, ice, gentle stretching, and over-the-counter pain relievers often help. Seek care if pain is severe, numbness develops, or symptoms do not improve in a week.
Poor Posture
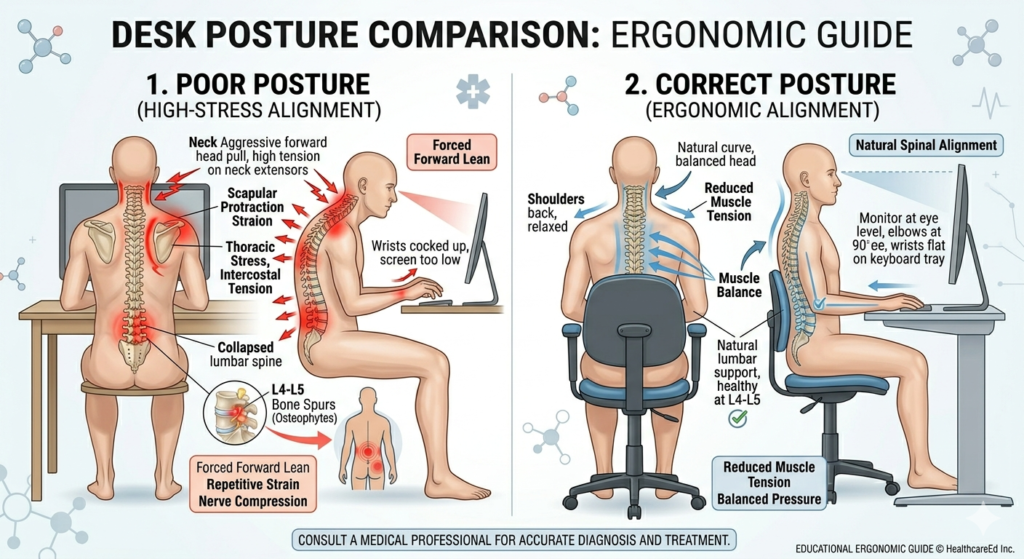
Poor posture puts steady strain on the muscles and ligaments of the upper back. Slouching at a desk, hunching over a phone, or sitting long hours without breaks shifts load onto the thoracic spine and shoulder girdle. You may feel a dull ache between the shoulder blades, stiffness, and reduced chest expansion.
Small changes reduce pain: adjust chair height, bring screens to eye level, and take frequent movement breaks. Strengthening exercises for the middle back and scapular stabilizers improve support. If posture-related pain persists despite these steps, a physical therapist can assess muscle imbalances and give tailored exercises.
Joint Dysfunction
Joint dysfunction in the upper back involves facet joints and costovertebral joints that link the spine and ribs. These joints can become irritated from repetitive motion, arthritis, or a minor injury. Pain often feels sharp with certain movements, such as deep breaths, twisting, or bending backward.
You might also notice limited range of motion and local tenderness over the joint. Treatment may include targeted mobilization, anti-inflammatory medications, and activity modification. In persistent cases, an imaging scan or referral to a spine specialist can identify joint degeneration or other structural issues.
Mid Back Pain: Key Contributing Factors
Mid-back pain often comes from structures in the thoracic spine, the ribs, or from long-standing spine shapes that change how your back handles load. You may feel sharp localized pain, aching between the shoulder blades, or pain that worsens with twisting, deep breathing, or prolonged sitting.
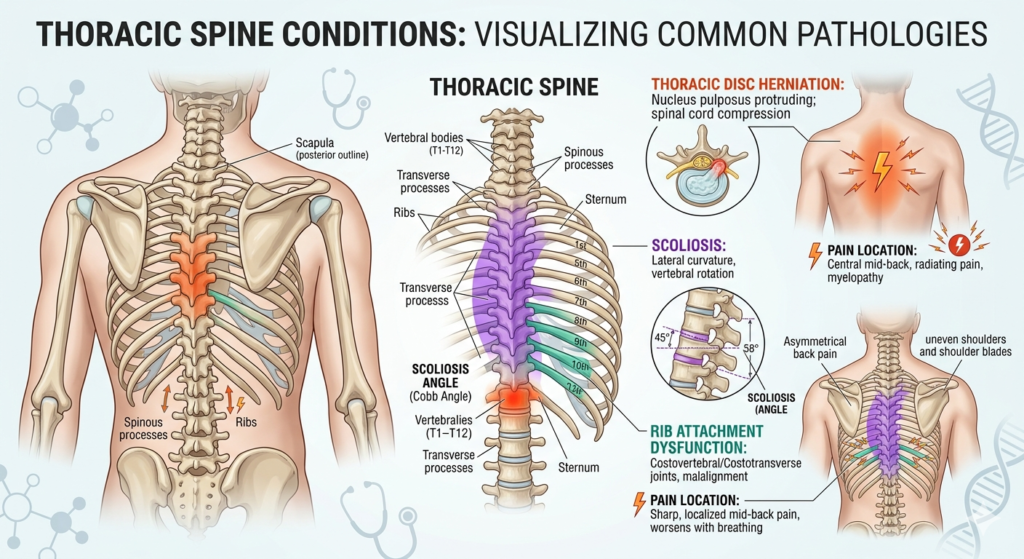
Thoracic Disc Issues
Degeneration, herniation, or bulging of thoracic discs can press on nerves or the spinal cord and cause localized or radiating pain. You might notice pain that gets worse when you bend forward, cough, or twist. Numbness, tingling, or weakness in the chest wall or along a rib level can appear if a nerve root is affected.
Diagnosing disc problems often involves MRI to view soft tissue and nerve compression. Treatment ranges from rest, anti-inflammatory medication, and physical therapy that targets posture and thoracic mobility, to steroid injections. Surgery is rare but may be needed for progressive neurological signs or severe cord compression.
Scoliosis and Structural Conditions
Scoliosis, kyphosis, and other structural spine changes alter load distribution across vertebrae and soft tissues. You may feel uneven muscle tightness, a persistent aching on one side, or pain after standing or walking for long periods. Structural changes can also lead to early disc wear or facet joint stress at specific levels.
You will often see asymmetric shoulder or rib height on exam. Imaging like X-rays shows curve severity and progression. Treatment focuses on bracing for adolescents, targeted exercise programs for adults, pain control, and, in severe cases, surgical correction to stabilize and realign the spine.
Rib Attachments
Pain at the thoracic spine can come from costovertebral or costotransverse joint irritation where ribs attach to vertebrae. You might feel sharp, tender pain that increases with deep breaths, coughing, or twisting. Palpation often reproduces the pain near the rib angles or along the back at specific levels.
Management includes manual therapy to mobilize the joint, stretching and strengthening of the paraspinal and rib stabilizer muscles, and anti-inflammatory measures. Local injections can provide diagnostic confirmation and temporary relief when conservative care fails.
Lower Back Pain: Common Triggers
You may feel sharp or dull pain, numbness, or stiffness in your lower back. These problems often come from specific structures like discs, joints, or nerves that change with injury or wear.
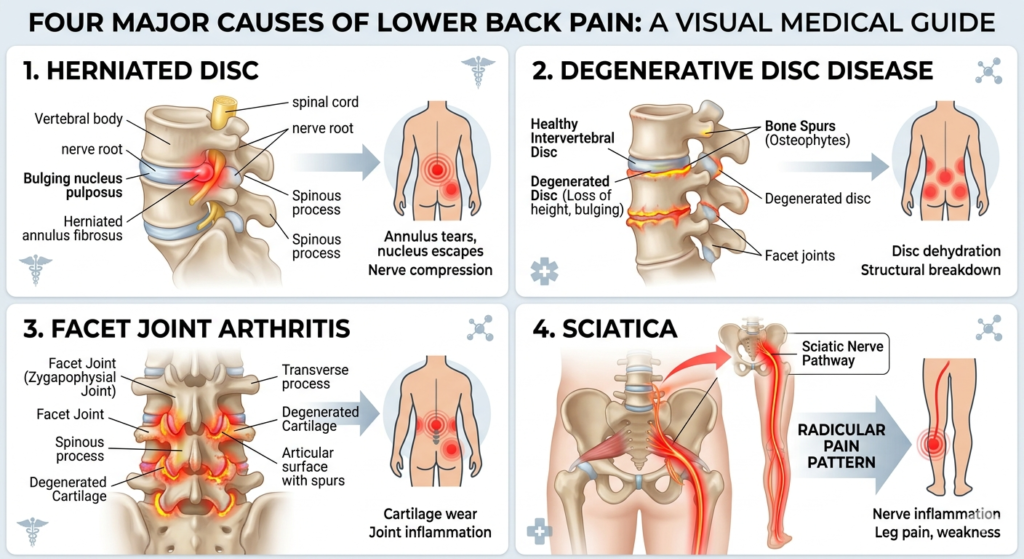
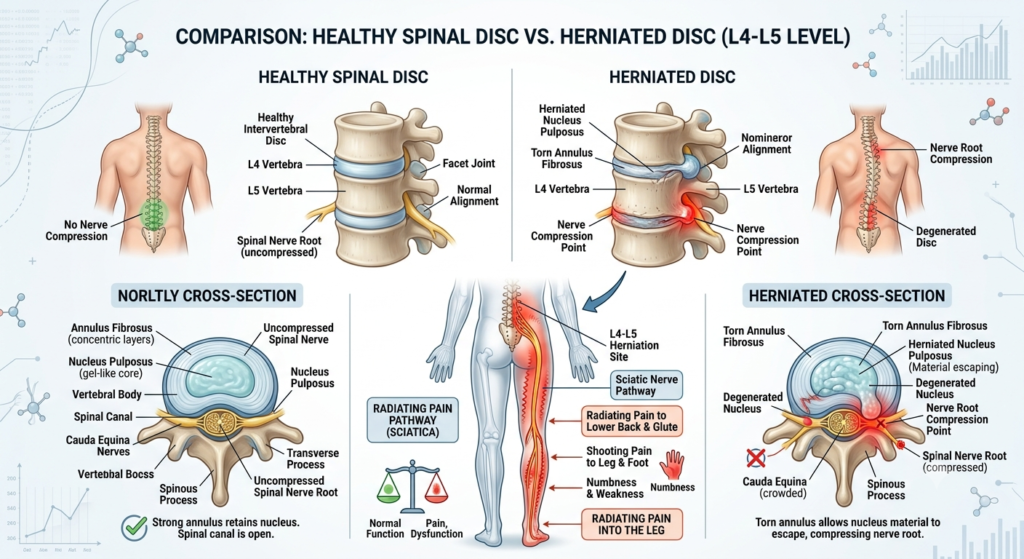
Herniated Discs
A herniated disc happens when the soft center of a spinal disc pushes through its outer layer and presses on nearby nerves. You might feel sudden sharp pain after lifting, twisting, or an awkward movement. Pain often radiates into one buttock or down a leg, and you may notice numbness, tingling, or muscle weakness in that leg.
Risk factors include heavy lifting, poor posture, and age-related wear. Diagnosis relies on your history, a physical exam, and sometimes MRI or CT scans. Treatment typically starts with rest, anti-inflammatory medication, physical therapy, and targeted exercises to reduce nerve pressure. If symptoms persist or you develop severe weakness, doctors may recommend steroid injections or surgery to remove the disc fragment.
Degenerative Disc Disease
Degenerative disc disease means the spinal discs lose height and cushioning over time. You may feel a deep ache in the lower back that flares with bending, lifting, or prolonged sitting. Pain often improves with movement or lying down, but can become chronic.
Wear-and-tear, reduced water content in discs, and small tears in the disc wall drive this condition. Smoking, repetitive strain, and genetics raise your risk. Diagnosis uses X-rays or MRI to show disc space narrowing and other changes. Treatment focuses on pain control with NSAIDs, core-strengthening exercises, and spinal stabilization techniques. In some cases, doctors suggest spinal injections, nerve ablation, or surgical fusion when conservative care fails.
Facet Joint Arthritis
Facet joint arthritis affects the small joints that connect vertebrae and guide spine movement. You will often feel localized pain near the spine that worsens when twisting or extending your back. Stiffness in the morning and pain when standing from sitting are common signs.
Arthritis develops from cartilage breakdown inside the facet joints due to aging, injury, or uneven spine mechanics. Imaging like X-rays or CT scans can show joint narrowing or bone spurs. Treatment includes physical therapy to improve flexibility, NSAIDs for pain, and heat or ice. For persistent pain, doctors may use steroid injections into the facet joints or radiofrequency ablation to block painful nerve signals.
Sciatica
Sciatica refers to pain that follows the path of the sciatic nerve from the lower back down the leg. You may feel sharp, burning pain or numbness that travels below the knee and into the foot. Symptoms are often worse with sitting, coughing, or sneezing.
Sciatica arises when the sciatic nerve becomes pinched by a herniated disc, bone spur, or spinal stenosis. A focused exam tests reflexes, muscle strength, and nerve stretch signs. Treatment usually involves rest, anti-inflammatories, and physical therapy that targets nerve gliding and core strength. If pain or weakness persists, your doctor might recommend epidural steroid injections or, in selected cases, surgery to relieve the nerve compression.
Pain Radiating to Other Areas
You may feel back pain that spreads to other parts of your body. The two main reasons are nerve signals that travel from the spine and nerves that refer pain to nearby areas.
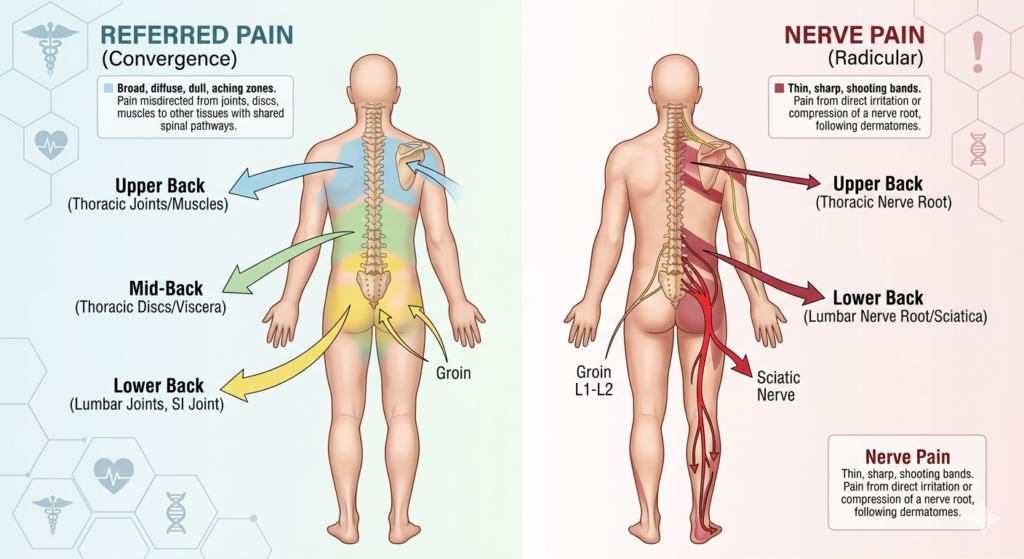
Referred Pain Patterns
Referred pain comes from tissues near the spine—muscles, ligaments, discs, or joints—but you feel it somewhere else. For example, a problem in your lower back can cause pain in your groin or buttock without nerve compression.
Common patterns:
- Low back → groin, front of thigh, or inner thigh.
- Mid back → chest or abdomen on the same side.
- Upper back → shoulder blade or chest.
You might notice the pain is dull, aching, or hard to pinpoint. Movement or pressure on a specific spinal segment often increases this type of pain. Referred pain usually does not follow a straight line down the leg like true nerve pain does.
Radiculopathy
Radiculopathy happens when a nerve root near the spine becomes compressed or irritated. This produces sharp, burning, or electric shock–like pain that follows the path of the nerve.
Key signs:
- Pain that radiates down the leg (sciatica) or arm depending on the level.
- Numbness, tingling, or muscle weakness along the nerve’s route.
- Pain often worsens with coughing, sneezing, or bending.
Causes include herniated discs, bone spurs, and spinal stenosis. Diagnosis uses your history, a focused neurological exam, and sometimes imaging like MRI. Treatment ranges from pain control and physical therapy to injections or surgery when weakness or severe loss of function appears.
Non-Musculoskeletal Back Pain Sources
Some medical problems outside muscles and bones can cause back pain. These causes often come with other signs like fever, blood in urine, vaginal bleeding, belly pain, or changes in bowel habits.
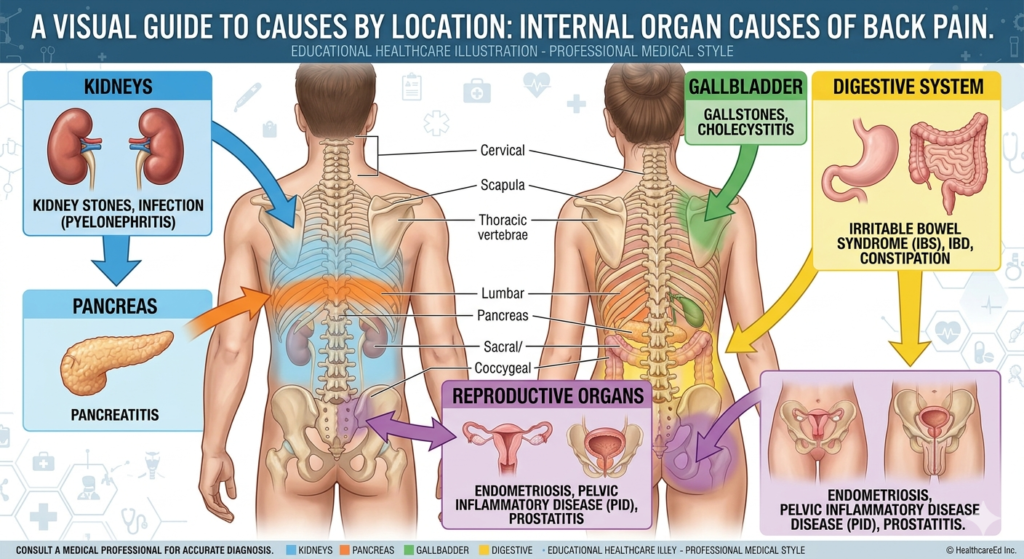
Kidney and Urological Causes
Kidney stones cause sharp, cramping pain that often starts in the side or back and may move toward your groin. You may also have blood in your urine, nausea, vomiting, and a strong urge to urinate. Fever usually means infection and needs prompt care.
Urinary tract infections (UTIs) that reach the kidneys (pyelonephritis) give steady, deep pain in the flank and lower back. You may notice fever, chills, cloudy urine, or burning with urination. Older adults may only show confusion or weakness.
Other urological problems like hydronephrosis (blocked urine flow) or kidney cyst rupture can produce sudden, severe back pain and reduced urine output. Seek evaluation if pain is intense, sudden, or comes with fever, fainting, or changes in urination.
Gynecological Factors
Uterine fibroids, ovarian cysts, endometriosis, and pelvic inflammatory disease can all cause back pain referred from the pelvic organs. Pain often sits low in the back and may worsen with menstruation, intercourse, or bowel movements.
Ectopic pregnancy gives sharp one-sided pelvic or back pain plus missed periods and vaginal spotting; this is an emergency. Ovarian torsion causes sudden, severe lower abdominal and back pain, nausea, and vomiting and needs urgent surgery.
Look for gynecologic signs with back pain: abnormal bleeding, heavy periods, pelvic pressure, or fertility issues. If you have these symptoms with severe or worsening pain, get prompt gynecologic evaluation.
Digestive System Disorders
Peptic ulcers, pancreatitis, gallbladder disease, and inflammatory bowel disease can refer pain to the back, usually the upper or middle back for pancreatic and gallbladder causes. You may also have nausea, vomiting, fever, or changes in bowel habits.
Pancreatitis causes severe, constant upper abdominal pain that radiates to the middle or upper back and often improves by leaning forward. Gallstones or cholecystitis give right-upper abdominal pain that can travel to the right shoulder blade or upper back, often after fatty meals.
Bowel problems like diverticulitis or large bowel obstruction can cause lower back pain along with fever, constipation, or bloody stools. Seek care if you have intense pain, fever, vomiting, or blood in stool.
Risk Factors and Prevention
Many things raise your chance of back pain, and some steps lower that risk. Focus on body weight, movement patterns, work setup, and health conditions that affect bones and nerves.
Lifestyle Influences
Smoking reduces blood flow to spinal discs and slows healing. If you smoke, quitting lowers your risk of chronic disc damage and speeds recovery after injury.
Being overweight adds steady pressure to your lower back. Losing 5–10% of body weight can cut strain and reduce pain for many people.
Sitting for long hours weakens core and hip muscles. Break up sitting every 30–60 minutes with 2–5 minutes of standing or walking. Use a chair with lumbar support and keep feet flat on the floor.
Lack of regular exercise makes muscles less able to support your spine. Aim for 2–3 sessions a week of core-strengthening and aerobic activity. Gentle stretching helps maintain flexibility.
Poor sleep position or a sagging mattress can keep back pain active. Sleep on a medium-firm mattress and use a pillow that keeps your neck aligned. Try side sleeping with a pillow between your knees.
Occupational Hazards
Jobs that lift heavy objects or require repeated bending raise injury risk. Use a two-person lift for items over 50 pounds. Bend at the knees, not the waist, and keep loads close to your body.
Prolonged standing or awkward postures strain the lower back. Use an anti-fatigue mat, alternate tasks, and change posture every 20–30 minutes when possible.
Repetitive twisting or vibration (e.g., driving heavy equipment) harms discs and ligaments. Limit continuous exposure, use vibration-damping seats, and schedule regular breaks.
Poor workstation ergonomics lead to neck and upper back pain. Position your monitor at eye level, keep elbows near 90 degrees, and use a chair with adjustable lumbar support.
Workplace training reduces injuries. Ask your employer for manual-handling training, ergonomic assessments, and access to lifting aids.
Underlying Health Conditions
Degenerative disc disease and osteoarthritis wear down spinal structures over time. Weight management, low-impact exercise, and physical therapy can slow progression and reduce symptoms.
Herniated discs press on nerves and cause sharp, radiating pain. Early activity modification, guided exercises, and, if needed, steroid injections often relieve symptoms without surgery.
Spinal stenosis narrows the canal and causes leg pain with walking. You can try activity pacing, core strengthening, and using a forward-leaning posture or a walker for relief.
Medical problems like osteoporosis increase fracture risk. Get bone density testing if you are postmenopausal, on long-term steroids, or have low body weight. Calcium, vitamin D, and medications help protect bone strength.
Infections, tumors, and inflammatory diseases are less common but serious. Seek prompt medical evaluation if you have fever, unexplained weight loss, or severe night pain.
Recognizing Signs of Serious Causes
You should watch for sudden, severe pain that does not improve with rest. This can signal a serious problem that needs quick care.
If you have numbness, weakness, or tingling in your legs, seek help right away. Loss of bowel or bladder control is an emergency and needs immediate medical attention.
Pay attention to pain after a fall, crash, or heavy lift. This raises the chance of fracture or damage to spinal structures.
Look for fever, unexplained weight loss, or night pain that wakes you. These signs may point to infection or cancer and require prompt testing.
Use this quick checklist to remember warning signs:
- Severe, sudden pain unrelieved by rest
- Numbness, weakness, or tingling in legs
- Loss of bowel or bladder control
- Recent trauma (fall, car crash)
- Fever, night pain, or unexplained weight loss
Tell your doctor about any of these signs. Early evaluation and imaging, when needed, can prevent worse problems.
When to Seek Professional Evaluation
If your pain is severe, lasts more than a few weeks, or gets worse despite home care, see a healthcare professional. Sudden, sharp pain after an injury needs immediate attention.
Watch for red flag symptoms like fever, unexplained weight loss, numbness, or weakness in your legs. These signs can point to infection, cancer, or nerve damage and require prompt evaluation.
Seek urgent care if you have bowel or bladder control problems or progressive leg weakness. These symptoms can indicate cauda equina syndrome, which is a medical emergency.
Use this quick checklist to decide whether to seek care:
- New or worsening pain after an accident
- Pain with fever or unexplained weight loss
- Numbness, tingling, or muscle weakness
- Loss of bowel or bladder control
Bring a clear history to your appointment: when the pain started, what makes it better or worse, and any recent injuries or illnesses. Also note past spine problems and current medications.
Expect your clinician to do a physical exam and ask targeted questions. They may order imaging (X-ray, MRI) or blood tests only when needed to confirm a diagnosis or rule out serious conditions.